
Deliberate Ignorance
Some idiot at The Atlantic is asking for amnesty for pushing bad Covid policies - because "we didn't know better." That's a load of alpaca doo-doo.


In case you missed it, some nitwit over at The Atlantic has written a self-serving piece of crap about how we need to declare an “amnesty” for all the bad things she supported in the name of Covid.
The main defense given in the screed is that we just didn’t know any better. But now that we do, it’s time to forgive the author and her fellow nutbags for turning into enthusiastic Gestapo officers, and let them get on with tormenting someone else. (The nitwit’s name is Emily Oster, and she’s also a professor of economics at Brown University so presumably the targets of her tormenting would be her own students.)
To respond to this idea of “amnesty” we’re taking a look at some of the willful ignorance involved in the Covid response - by reading the 2019 WHO report1 on the use of non-pharmaceutical interventions (NPIs) to reduce the transmission of influenza (and other respiratory diseases).
The report looks at 18 different interventions and recommends using most of them - despite almost no existing evidence that any of them work. We’ll see the decision making of supposed experts, as they used the absence of data as an excuse to recommend actions, the opposite of what good science, and government policy, should be.
First, a quick review on the theory behind using NPIs
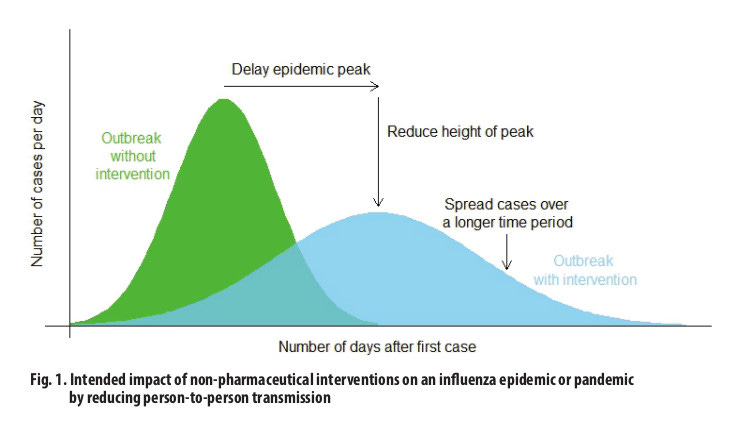
Reducing transmission is the phrase they use constantly. This doesn’t mean you don’t get sick. It mostly means that it might take longer for everyone to get sick, so we won’t overflow hospitals and will have time to develop pharmaceutical interventions. Whether fewer people actually get sick is a great, big maybe. But the evidence doesn’t support that conclusion.
I have a short article explaining this concept, and the even shorter version of that already short explanation is that this chart from the report shows the same number of people getting sick, whether the non-pharmaceutical interventions work or not.
Once we’re past the peak, and have vaccines that we’re told work, then we’re supposed to be done with these measures. This isn’t some great, hidden secret - it’s part of the introduction of the WHO report. Did I mention this report is available online, for free?
The evidence, and the quality of that evidence
Below are short summaries of the 18 types of NPIs in 15 categories, reviewed in the WHO report. For each summary I made a small table (adapted from the big table in the report) listing what the evidence generally shows (“Balance of Evidence”), the quality of that evidence, and the WHO recommendation. On quality of evidence, the report authors tell us:
In general, randomized controlled trials (RCTs) provided the strongest evidence, followed by observational studies and then computer simulations.
Only two categories on the whole list have enough evidence to rise to the level of “moderate” and the evidence for both of those is that they don’t work. Those two items have actual RCTs to reference, and account for 21 of the whopping total of 23 RCTs use in the report. For everything else, the evidence is anywhere from poor to non-existent.
As a result the word “plausible” gets a serious workout in this report. We’re often told it’s plausible that something will work, although there’s no evidence that it does. The WHO authors recommend many of the interventions based purely on plausibility. In fact they recommend most things, despite almost no evidence any of it works.
Hand hygiene

This is one of the two categories with actual clinical data, and 11 Randomized controlled trials (RCTs) were included in the analysis.
Full Recommendation Quote:
Hand hygiene is recommended as part of general hygiene and infection prevention, including during periods of seasonal or pandemic influenza. Although RCTs have not found that hand hygiene is effective in reducing transmission of laboratory-confirmed influenza specifically, mechanistic studies have shown that hand hygiene can remove influenza virus from the hands, and hand hygiene has been shown to reduce the risk of respiratory infections in general.
It’s entirely possible that all these studies have told us is that we already do a decent job of washing our hands. The good news about this category is that no one ever suggested staffing toilets with people who forcibly wash our hands for us. A small blessing, but we’ll take it.
Respiratory etiquette

There’s no evidence on this at all - maybe it helps, or maybe sneezing puts enough pathogens into the air that it doesn’t matter what we do. But remember that plausible is the minimum bar for recommendation by the WHO, so we’ll stick plastic shields everywhere anyway.
Full Recommendation Quote:
Respiratory etiquette is recommended at all times during influenza epidemics and pandemics. Although there is no evidence that this is effective in reducing influenza transmission, there is mechanistic plausibility for the potential effectiveness of this measure. (emphasis added)
Personally, I don’t sneeze on people because it’s rude. But that’s just me.
Face masks

The authors looked at 10 randomized controlled trials, including more than 6,000 participants. Keep in mind that not every review (like this report) will include all studies - the authors set their own inclusion criteria.
There were a total of 18 RCTs with masks published between 2008 and 2019, including the 10 the authors referenced. If you want to look at all 18, I have another article summarizing them. The short version is that there’s almost no evidence they work, and a little bit of evidence they might do harm.
Full Recommendation Quote:
Face masks worn by asymptomatic people are conditionally recommended in severe epidemics or pandemics, to reduce transmission in the community. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure. (emphasis added)
There’s that word again - plausible. Although clinical trials consistently fail, because some lab tests show viruses being filtered they go ahead and recommend masks anyway.
A disposable surgical mask is recommended to be worn at all times by symptomatic individuals when in contact with other individuals. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure. (emphasis added)
The WHO authors didn’t look for evidence of harm (like reduction in oxygen or increase in carbon dioxide, which I found easily) and ignore the worrisome results in some of the published studies.
Once again, there’s no evidence they work, but they’re recommended anyway. Well, but not cloth masks:
Reusable cloth face masks are not recommended. Medical face masks are generally not reusable, and an adequate supply would be essential if the use of face masks was recommended. If worn by a symptomatic case, that person might require multiple masks per day for multiple days of illness.
So they say not to wear reusable cloth masks, but professors at Brown University apparently can’t be bothered to read this far into a report that has so few pictures. Tell me how anyone justified mandates for cloth masks based on any of this data. I’ll wait.
Surface and object cleaning

Two RCTs and one cross-sectional study were included. Just like with hand hygiene, it’s possible the normal amount of household cleaning is already sufficient to get the maximum benefit.
Full Recommendation Quote:
Surface and object cleaning measures with safe cleaning products are recommended as a public health intervention in all settings in order to reduce influenza transmission. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure.
Once again, it’s recommended because it’s plausible, not because anyone ever showed it works. So let’s scrub the world with bleach.
Other environmental measures

For UV and humidity, they found no studies. For improved ventilation, the only evidence is from a small number of simulation studies. It’s curious they list it as effective when the only data is from simulations. (A simulation isn’t evidence of anything besides the inputs and algorithms of the simulation. If the inputs are wrong the results are useless.)
Full Recommendation Quote:
Installing UV light in enclosed and crowded places (e.g. educational institutions and workplaces) is not recommended for reasons of feasibility and safety.Grading of Recommendations Assessment, Development and Evaluation (GRADE)
I’m almost relieved to find the authors have some limits, but it’s not really surprising that they would be concerned about blasting people with UV in the absence of strong evidence. How about ventilation?
Increasing ventilation is recommended in all settings to reduce the transmission of influenza virus. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure.
This is an interesting contradiction. After telling us there’s no evidence improving ventilation is effective, their own table lists it as effective. I’m not sure which they think is correct, however this sounds like a reason to have people go outside, not lock them in their homes.
And for humidity:
There is no evidence that modifying humidity (either increasing humidity in dry climates, or reducing humidity in hot and humid climates) is an effective intervention, and this is not recommended because of concerns about cost, feasibility and safety.
One of the few things in the report listed as effective (improved ventilation) is something reduced by another one of the Covid policies - telling people to stay in their homes.
Contact tracing

Four simulation studies were included, but none of them looked at just contact tracing by itself.
Full Recommendation Quote:
Active contact tracing is not recommended in general because there is no obvious rationale for it in most Member States. This intervention could be considered in some locations and circumstances to collect information on the characteristics of the disease and to identify cases, or to delay widespread transmission in the very early stages of a pandemic in isolated communities.
So the WHO, in their great big report, said there’s no rationale for contact tracing. But we tried to do it anyway. Because our dear leaders follow the experts’ advice when it’s what they already wanted to do, and ignore that advice when it’s not.
Note for incompetent faux-journalists: this is an example of when journalists are expected to do their jobs.
Isolation of sick individuals

The authors used four epidemiological studies and 11 simulation studies.
Full Recommendation Quote:
Voluntary isolation at home of sick individuals with uncomplicated illness is recommended during all influenza epidemics and pandemics, with the exception of the individuals who need to seek medical attention. The duration of isolation depends on the severity of illness (usually 5–7 days) until major symptoms disappear. (emphasis added)
Big surprise, the thing we already do normally (keep sick kids home from school) is probably useful. And even the folks at the WHO thought it would only be voluntary.
In China this was apparently interpreted to mean getting marched to the gulag if you have a two degree temperature. Sorry, I meant China, Australia and New Zealand.
Quarantine of exposed individuals

They found six epidemiological studies and 10 simulation studies to include. Some of these were quarantines at home, some at borders or on ships. Sometimes other interventions were also being used.
Home quarantine of exposed individuals to reduce transmission is not recommended because there is no obvious rationale for this measure, and there would be considerable difficulties in implementing it.
So the WHO recommended against locking people in their homes. But only because they thought it would be hard to do - of course they didn’t count on the nascent authoritarianism present in so many governments. They have a very low bar for what is effectively house arrest.
Some countries chose to combine this one with the previous intervention and build quarantine camps for both symptomatic people and those who were simply exposed to a symptomatic person - true totalitarian efficiency.
School measures and closures

Measures (desk spacing, staggering recess, etc.) and closures are listed together as a single item to evaluate. At least this time there were lots of papers to read:
A systematic review published in 2013 identified 79 epidemiological studies on school closures, and summarized the evidence as demonstrating that this intervention could reduce the transmission of pandemic and seasonal influenza among school children; however, the optimum strategy (e.g. length of closure, and whether it should be reactive or proactive) remained unclear, owing to heterogeneity of the data. The current systematic review updated the 2013 review, identifying 22 additional epidemiological studies that met the inclusion criteria, giving a total evidence base of 101 studies.
But no RCTs at all, and the authors rate the quality of evidence here as very low. Here’s their full recommendation:
School measures (e.g. stricter exclusion policies for ill children, increasing desk spacing, reducing mixing between classes, and staggering recesses and lunchbreaks) are conditionally recommended, with gradation of interventions based on severity. Coordinated proactive school closures or class dismissals are suggested during a severe epidemic or pandemic. In such cases, the adverse effects on the community should be fully considered (e.g. family burden and economic considerations), and the timing and duration should be limited to a period that is judged to be optimal.
That part about “timing and duration should be limited” went right out the window when teachers unions realized they could get paid to stay home. Government officials ignored the limitations while the laptop class cheered their policies - and both sent their kids to private school.
This alone is justification to disregard the plea for amnesty.
Workplace measures and closures

The authors included seven epidemiological studies and 12 simulation studies in their review. They’ve lumped “measures” and “closures” together again, and the recommendations for each are slightly different.
Full Recommendation Quote:
Workplace measures (e.g. encouraging teleworking from home, staggering shifts, and loosening policies for sick leave and paid leave) are conditionally recommended, with gradation of interventions based on severity. Extreme measures such as workplace closures can be considered in extraordinarily severe pandemics in order to reduce transmission.
Just like with keeping kids home from school, letting sick employees stay home might reduce transmission of disease. Of course, this is something we already do normally.
But also notice the main idea here isn’t closing businesses. Letting people work remotely, loosening the rules a bit on sick leave, etc. are conditionally recommended, and closing businesses is the last thing on the list, reserved for only the most severe of circumstances.
But journalists and college professors were getting paid regardless, so once again all the potential issues are simply ignored.
Avoiding crowding

The entire set of papers for this was three epidemiological studies.
Full Recommendation Quote:
Avoiding crowding during moderate and severe epidemics and pandemics is conditionally recommended, with gradation of strategies linked with severity in order to increase the distance and reduce the density among populations.
This is a good time to look at what “epidemiological studies” means. I actually used this specific category in the article Desperate measures as an example of how poor the quality of the research can be. Those “studies” consisted of two papers about the 1918 flu epidemic (written 90 years later) and one paper about kids sleeping in a gym.
No one has any idea if avoiding crowding does anything, but they’re still going to give it a conditional recommendation. Unless of course you’re out protesting something The Atlantic editors agree with, in which case you just go crazy, kid. Burn down a Wendy’s while you’re at it.
Travel advice

This is advice to travelers - not telling them where they can and can’t go, not restricting their movements - just giving them information. We’re lucky no one came up with a way to abuse this one too. (“You must read this and pass a short quiz before we let you travel!”)
Full Recommendation Quote:
Travel advice is recommended for citizens before their travel as a public health intervention in order to avoid potential exposure to influenza and to reduce the spread of influenza.
Entry and exit screening

Ten articles were used, mostly observational studies.
Full Recommendation Quote:
Entry and exit screening for infection in travellers is not recommended, because of the lack of sensitivity of these measures in identifying infected but asymptomatic (i.e. pre- symptomatic) travellers.
In the notes for this item (later in the report) they state:
There is a very low overall quality of evidence that entry and exit screening can delay the introduction of infection to a country and local transmission.
The most they suggest is a brief delay in the virus being introduced to the country, then everyone gets sick anyway. So why bother at all?
Internal travel restrictions

One epidemiological study and four simulation studies.
Full Recommendation Quote:
Internal travel restrictions are conditionally recommended during an early stage of a localized and extraordinarily severe pandemic for a limited period of time. Before implementation, it is important to consider cost–effectiveness, acceptability and feasibility, as well as ethical and legal considerations in relation to this measure.
Four of the five studies are just simulations, not real world data. The one actual study showed a relationship between air travel and when the flu season peaks, but not a reduction in how many people got sick. So once again “effective” just means you get sick later.
Border closure

Two epidemiological studies and nine simulation studies.
Full Recommendation Quote:
Border closure is generally not recommended unless required by national law in extraordinary circumstances during a severe pandemic, and countries implementing this measure should notify WHO as required by the IHR (2005).
Once again, lots of people seemed to decide their circumstances were “extraordinary” enough to justify this, despite almost no evidence it does anything.
Some closing thoughts
There are very few papers on non-pharmaceutical interventions. Out of the many millions of published papers in the scientific literature, subjects like border closures or isolating sick people have just a handful of papers. And this whole report only discusses 23 randomized controlled trials.
But the word “plausible” destroyed lives and livelihoods. Anyone claiming to work in journalism or academia could have looked at this, and other sources of data, and quickly realized how outrageous the proposed policies were - masks, lock downs, school and business closures, etc.
Not knowing isn’t the same as refusing to learn, especially when your job is specifically to research and explain things.
But the author, and everyone like her, chose deliberate ignorance.
The rest of us will not discuss forgetting, or forgiving, until there has been a loud and clear admission of this.
By the way, the recommendations in this report came from a group meeting in China:
A technical consultation meeting for the development of this guidance was held in Hong Kong Special Administrative Region (SAR), China, on 26–28 March 2019.
Is it at all shocking that the authors recommend so many interventions on so little evidence?

Latest version of WHO report:
https://apps.who.int/iris/bitstream/handle/10665/329438/9789241516839-eng.pdf
Archived copy from 2020 at the Internet Archive:
https://web.archive.org/web/20200330124252/https://apps.who.int/iris/bitstream/handle/10665/329438/9789241516839-eng.pdf
Original location, now defunct:
Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza; World Health Organization 2019. ISBN: 978-92-4-151683-9.
https://www.who.int/influenza/publications/public_health_measures/publication/en/
Just wait for fallout that will come to light over the next couple months and years.
Great article John, however I think we should understand they aren't really *asking* for forgiveness or amnesty, they're publicly forgiving themselves.
No amnesty.
No quarter.
Never forget.