

There's no such thing as virus free
There's no such thing as virus free
Sometimes scientists do something clever, and we all learn something useful.

It seems some people have the impression that we all go through life free of viruses, bacteria and fungi until one day - BAM! We’re exposed to some nasty little pathogen and are now spending the day on the couch watching old movies like Rudy Ray Moore’s 1975 film masterpiece Dolemite.
[Warning: either a fever or a lot of alcohol is recommended prior to watching this movie. It makes Zombeavers1 look like an art film.]
Getting back to viruses: if it were true that we’re virus free until exposed to someone infectious, then simply isolating oneself would guarantee an illness-free cold and flu season. But it turns out this isn’t the case, and sometimes even people in isolation will spontaneously develop respiratory infections.
This isn’t something new and researchers have been discussing and documenting examples for decades. Here’s a fun one, from back in the days of disco and Dolemite:
An outbreak of common colds at an Antarctic base after seventeen weeks of complete isolation (Allen et al. 19732)
This paper describes a spontaneous outbreak of colds at an isolated base in Antarctica. You know, the kind of secret government base that no one knows exists until some idiot uploads Fitbit data to Strava3.
[Strava released heat maps showing where people exercise, and sharp observers noticed that one of the jogging routes was in Antarctica4 where there are no visible above ground structures. There appear to be sets of straight, interconnected underground corridors that someone has been using as an indoor track.]
Back to 1973:
The staff at the base had no outside contact for about 4 months, but half of them got sick anyway (actually diagnosed sick, not just trying to get out of jogging laps).
Six of 12 men wintering at an isolated Antarctic base sequentially developed symptoms and signs of a common cold after 17 weeks of complete isolation. Examination of specimens taken from the men in relation to the outbreak has not revealed a causative agent.
The paper’s authors discuss how remote bases like this one provide an opportunity to study spontaneous outbreaks, so the personnel at the base were being monitored for respiratory infections.
During the preliminary observation period, after 17 weeks of isolation, upper respiratory symptoms occurred in one man and then spread to half the Base complement over the next week in the manner of an infectious disease. No virus had been artificially introduced at this time, and the outbreak was unexpected.
So nothing for 17 weeks, then one guy gets sick and infects half the staff. The authors suspected a viral cause, probably rhinovirus, because it’s very common and causes many upper respiratory infections.
However, no studies of antibody against rhinovirus could be attempted, because of the multiplicity of serotypes, yet these viruses are thought to produce up to 50-60 % of upper respiratory infections in adults (Rhodes & van Rooyen, 1968), and could have been responsible for this
outbreak.
This all suggests that someone at the base had a virus, probably rhinovirus (HRV) already in his system, and this developed into an infectious cold.
Thirty-five years later some researchers in another place with a reputation for chilly temperatures (Finland) published a paper that supports this idea.
Identification of respiratory viruses in asymptomatic subjects: asymptomatic respiratory viral infections (Jartti et al. 20085)
The authors of this paper did something interesting. In 2008 polymerase chain reaction (PCR) testing was still somewhat new, but also much more sensitive than other methods of detecting viruses. But rather than looking at the symptomatic subjects, the authors reviewed a group of studies and cataloged the test results of the asymptomatic subjects.
The medical literature of the past 4 decades was searched regarding respiratory virus detection by polymerase chain reaction and conventional methods (culture, antigen detection, serology) in asymptomatic subjects in an attempt to determine the prevalence and clinical significance of such viruses in normal persons.
Here is a small chart (mine, not theirs), summarizing some of their findings:
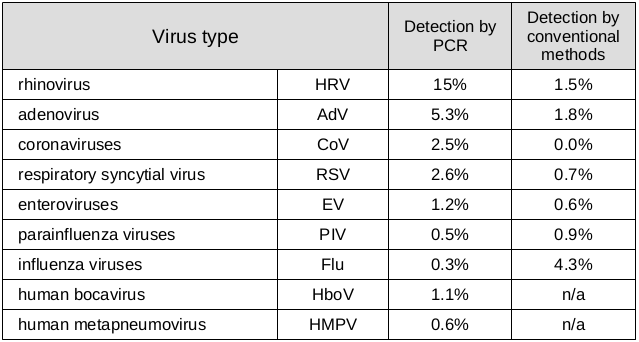
Of healthy subjects in the various studies, an average of 15% had detectable rhinovirus in their bodies and various lesser numbers of people had other common viruses. So it’s believable that not one, but two, of the people at the base in Antarctica were carrying rhinovirus.
There is some overlap - in some cases subjects had more than one respiratory virus, so we can’t just add all these up to get the total number of people with detectable respiratory viruses. But whatever the total is, clearly that number is significant.
What do these results mean? The authors give us a few possibilities:
1. symptomatic infection but symptoms/signs are not recognized;
2. asymptomatic infection (acute, persistent or reactivation of latent infection), ie, without associated signs/symptoms;
3. incipient infection, ie, symptoms have not yet developed;
4. past infection, ie, PCR detects remnants of distant infection.
Many of us are probably walking around (jogging, even) with respiratory viruses in our systems even though we have no symptoms.
It seems that both RNA and DNA viruses are able to cause persistent or smoldering infections (ie, viral replication occurs with or without symptoms long after the initial viral illness). In contrast to RNA viruses, DNA viruses can also stay latent in the airway tissues (ie, viral proteins are produced without replication of a complete virus). Latent infection may occur after an acute replicating infection if viral DNA forms an episome within the host cell or actually integrates into the host cell genome.
And apparently some viruses can just remain, latent, in airway tissues for an unknown length of time. The authors of this paper aren’t the only researchers who have noted a significant percentage of asymptomatic infections.
Human rhinoviruses (Jacobs et al. 20136)
This paper is an overview of human rhinovirus (basic virology, pathogenesis, epidemiology, etc) and they note that HRV is found in asymptomatic children - and in a large percentage of them.
With the increasing use of molecular methods of viral detection, asymptomatic HRV infection has been noted to be relatively common, particularly in children.
The rate of asymptomatic infection is consistent with what the authors in the Jartti paper found.
In children less than 4 years old, rates of asymptomatic infection range from 12 to 32% and tend to be higher in the youngest age groups.
Cool. But why am I bringing this up now?
First, because it’s interesting. Being “healthy” doesn’t necessarily mean being free of all pathogens. Viruses can (and do) hang around, waiting for something to temporarily weaken our immune systems and giving them an opportunity to grow and spread. Being healthy really means having an immune system that handles these pathogens, all the time.
Second (and perhaps more importantly) - remember the post summarizing the randomized controlled trials of masks, where the masked groups sometimes got sick more than the control groups? People had fevers and sore throats, but not from influenza virus. Some of those could have simply been the common cold.
The Jacobs paper gives us some more background on HRV. Infection often starts in the sinuses or the mucous membranes under the eyelid.
HRVs are transmitted from person to person via contact (either direct or through a fomite) or aerosol (small or large particle). HRV infection is efficiently initiated by intranasal and conjunctival inoculation but not by the oral route.
And from there, it can move into the lower airway, possibly leading to a lower respiratory infection.
Gern et al. experimentally infected eight adult allergic volunteers with HRV-16. All subjects developed cold symptoms and had HRV-16 cultured from nasal specimens. In addition, in all subjects, HRV-16 was detected by reverse transcription-PCR (RT-PCR) in lower airway cells obtained via bronchoalveolar lavage (BAL) at 2 to 4 days following infection.
Those masks, of course, are trapping any virus shed from the sinuses or upper respiratory tract right where they need to be to cause a fresh infection. The insides of those masks could contain more pathogens than the outsides.
So in those mask studies, what sounded impossible (more people in masks being ill) starts to look more plausible. No one has tried to explain those results, but is it possible the masks were helping some other, already present virus, to flourish?
Health authorities have, without evidence, convinced many people to lock themselves in their homes, avoid human contact, and dress like some kind of bizarre pod people who fear the feel of fresh air on their faces.
If they had educated us instead, many of us would be much more pragmatic about health decisions and would look more at the potential harms of these various health measures. Of course that may be the reason they opted for the fear.
Dolemite has reached it’s… interesting conclusion and the credits are rolling. They are giving special thanks to the following groups:
THE NEW TOTAL EXPERIENCE
MR. FAT BURGER
CHUCK NORRIS KARATE SCHOOL
WILSON HILL and RACHAL MORTUARY
THE GEISHA HOUSE OF BEAUTIFUL WOMEN
BILL COUSER AND HIS DANCERS
I have that same feeling I get whenever I read new pronouncements from the CDC. Is this intended to be serious, or are we being trolled?
https://www.imdb.com/title/tt2784512/
Allen TR, Bradburne AF, Stott EJ, Goodwin CS, Tyrrell DA. An outbreak of common colds at an Antarctic base after seventeen weeks of complete isolation. J Hyg (Lond). 1973;71(4):657-667. doi:10.1017/s0022172400022920
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2130424/
Story about Strava and Fitbit data showing secret bases:
https://www.popularmechanics.com/technology/apps/a15912407/strava-app-military-bases-fitbit-jogging/
Archived copy:
https://web.archive.org/web/20210313183504/https://www.popularmechanics.com/technology/apps/a15912407/strava-app-military-bases-fitbit-jogging/
Reddit shows location of Anatarctic base:
https://www.reddit.com/r/CosmicDisclosure/comments/9exnzl/antarctica_base_proof_via_google_earth_strava/
Archived copy:
https://web.archive.org/save/https://www.reddit.com/r/CosmicDisclosure/comments/9exnzl/antarctica_base_proof_via_google_earth_strava/
Jartti T, Jartti L, Peltola V, Waris M, Ruuskanen O. Identification of respiratory viruses in asymptomatic subjects: asymptomatic respiratory viral infections. Pediatr Infect Dis J. 2008 Dec;27(12):1103-7. doi: 10.1097/INF.0b013e31817e695d. PMID: 18978518. https://pubmed.ncbi.nlm.nih.gov/18978518/
Jacobs SE, Lamson DM, St George K, Walsh TJ. Human rhinoviruses. Clin Microbiol Rev. 2013 Jan;26(1):135-62. doi: 10.1128/CMR.00077-12. PMID: 23297263; PMCID: PMC3553670.
https://pubmed.ncbi.nlm.nih.gov/23297263/