

Nate the Pneumonia Gnome
Nate the Pneumonia Gnome
I thought I knew what pneumonia was, and I was very, very wrong.

Apologies in advance for what is going to be a pretty boring read.
We’re talking about an illness, and even Nate the Pneumonia Gnome can’t make this interesting. He’s done a lot of public service announcements but, just like Julie Andrews on the set of The Sound of Music, he was drunk most of the time.
Given how excited everyone seems to be about the Rona, Nate thought it might be a good idea to review some CDC mortality data1. This partial screenshot comes from the CDC page on COVID-19 mortality:
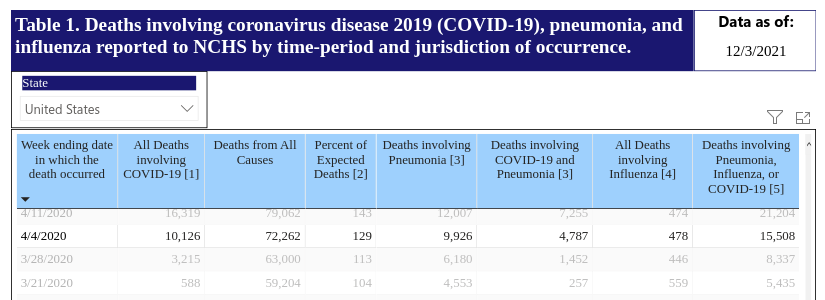
[1] Deaths with confirmed or presumed COVID-19, coded to ICD–10 code U07.1.
[3] Counts of deaths involving pneumonia (J12.0-J18.9) include pneumonia deaths that also involve COVID-19 and exclude pneumonia deaths involving influenza.
[4] Counts of deaths involving influenza (J09-J11) include deaths with pneumonia or COVID-19 also listed as a cause of death.
[5] Deaths with confirmed or presumed COVID-19, pneumonia, or influenza, coded to ICD–10 codes U07.1 or J09–J18.9.
The footnotes are less than enlightening. COVID-19 was originally described2 as a new type of pneumonia of unknown cause, and it turns out this innocuous sounding statement is significant.
The categories in the CDC database use something called ICD codes. ICD-10 is the latest version (I’ll go out on a limb here and guess that it’s the tenth) of the International Classification of Diseases and there are over 70,000 different codes. For the pneumonia and influenza listed in the footnotes there are 52 codes, which is 41 more than Nate has toes. Nate has issues.
COVID-19 has an ICD code for when the SARS-CoV-2 virus is detected or suspected in a pneumonia case (J12.82 Pneumonia due to coronavirus disease 2019). The guide3 for ICD codes says to code U07.1 first when using J12.82, which is footnote [1] in the screenshot. (Codes starting with U are special purpose codes for new diseases and Gnome-related incidents.)
And although COVID-19 is described as a type of pneumonia, some of the deaths in the table are listed as COVID-19 but not pneumonia, so there may be some other comorbidity involved. Nate is only the spokes-gnome for pneumonia so he’s not sure about those other deaths.
So this CDC table is a bit confusing, but since we have Nate’s help today we’re going to focus on the pneumonia cases. Anyone with suspected or confirmed SARS-CoV-2 virus gets coded as U07.1, then J12.82 if they are also diagnosed with pneumonia due to COVID-19, or one of the other codes if they have pneumonia due to another pathogen.
And this is where things get interesting.
Community-Acquired Pneumonia in Adults: Diagnosis and Management (Kaysin and Viera 20164)
More often than not, we don’t know the specific pathogen causing pneumonia in a particular patient (some of those ICD codes are for unknown or unspecified organisms).
Commonly used diagnostic methods may identify a pathogen in only 30% to 40% of patients.
And this was written in 2016! But we might be able to do better in the future:
Recent developments allow use of rapid multiorganism polymerase chain reaction– based testing for pathogen-directed treatment, with bacterial and viral detection rates as high as 86%.
So PCR testing of pneumonia patients only began recently, and might have high viral detection rates. (But also can have high rates of false positives, something to be discussed at a later date.)
Everybody seems to agree, we kinda suck at figuring out what causes a specific patient’s pneumonia:
Evolving Understanding of the Causes of Pneumonia in Adults, With Special Attention to the Role of Pneumococcus (Musher, Abers, and Bartlett 20175)
Recent studies fail to identify a causative organism in more than 50% of cases, which remains the most important challenge to understanding lower respiratory infection.
The authors have surveyed the literature and provided a list of etiological agents (the pathogens that caused the pneumonia), including things like Streptococcus pneumoniae, Haemophilus, Staphylococcusaureus, Rhinovirus, Coronavirus, Influenza, fungi, and others. For over half the patients the pathogen was unknown.
And unfortunately, just because you find a virus doesn’t always mean you’ve found the cause of the pneumonia.
Community-acquired pneumonia: An overview (Mandell 20156)
Lots of healthy adults carry respiratory viruses:
With the advent of polymerase chain reaction (PCR), the detection of viruses in respiratory samples has increased significantly and in some studies viruses have been found in up to one-third of adult CAP patients. The presence of a virus, however, does not prove causality as nasopharyngeal swabs can yield respiratory viruses in 20–30% of healthy adults.
Nate would like to convey his apologies to all the germophobes out there. We assume none of you are sleeping tonight, after that little revelation.
This leads us to an important little detail:
For now, keep in mind that the ICD code U07.1 means “confirmed or presumed COVID-19.” So there’s no guarantee that the pathogen was confirmed, which, given what we just learned about pneumonia, should now come as no surprise to us.
Wait, back up. What exactly is pneumonia, anyway?
Nate had to run to the liquor store, so we’ll turn to the NIH7 for a brief definition of pneumonia:
Pneumonia is an infection that affects one or both lungs. It causes the air sacs, or alveoli, of the lungs to fill up with fluid or pus. Bacteria, viruses, or fungi may cause pneumonia.
Well that was amazingly non-specific. Nate claims this is just the result of government employees being their usual less-than-useful selves, but it turns out pneumonia is a tricky illness.
So off we go into the scientific literature. Here’s another short definition from Pneumonia in the Immunocompetent Patient8:
Pneumonia is the acute inflammation of the lower respiratory tract and lung parenchyma resulting in a clinical syndrome of fever, cough, shortness of breath and malaise.
Now we have to look up parenchyma9:
Although often used to refer solely to alveolar tissue, term describes any form of lung tissue including bronchioles, bronchi, blood vessels, interstitium, and alveoli.
Okay, so pneumonia is a fairly broad term used to cover infection or inflammation of the lung tissue. But what causes it? Based on all the ICD codes it’s probably lots of things, and since Nate is now slurring his speech we must rely again on the available scientific literature.
Pneumonia has its own journal! (but no licensing deal with Nate)
Pneumonia is such an important topic that there’s an entire journal about it, which in a bout of unrestrained creativity (or merciful brevity) the founders chose to call Pneumonia. They recently published a short commentary to try and, um, clarify things for us.
The definition and classification of pneumonia (Mackenzie 201610)
After publishing an issue entirely about the diagnosis of pneumonia, they all decided that pneumonia itself is not really well defined.
A number of members of the Pneumonia Editorial Board engaged in a discussion and were in agreement that the lack of an accepted and widely used definition or classification of pneumonia is a significant problem.
If people who work at a journal called Pneumonia can’t agree on a definition, the rest of us are screwed. There are some bits in there about a dead guy named Hippocrates but let’s just skip to the textbook definition of pneumonia:
Harrison’s textbook of internal medicine defines pneumonia as an infection of the pulmonary parenchyma caused by various organisms. It states that pneumonia is not a single disease but a group of specific infections, each with a different epidemiology, pathogenesis, presentation and clinical course.
Did you get that? There are a bunch of different pathogens, that require differing treatments, that are lumped under the term pneumonia. The point of commonality is the lungs.
The editors eventually give us their recommendation for how to define pneumonia, which is consistent with the NIH. Maybe the NIH copied it from them, just like Nate and I are doing. He’s a drunk, lazy gnome.
Pneumonia should be defined as an acute infection of the lung parenchyma by one or co-infecting pathogens, but excluding the well-defined condition of bronchiolitis, the primary cause of which is almost always a viral agent.
Just for the hell of it, let’s check in with the CDC
The CDC actually divides pneumonia11 up into three categories:
Community-acquired pneumonia is when someone develops pneumonia in the community (not in a hospital). Healthcare-associated pneumonia is when someone develops pneumonia during or following a stay in a healthcare setting. Healthcare settings include hospitals, long-term care facilities, and dialysis centers. Ventilator-associated pneumonia is when someone gets pneumonia after being on a ventilator, a machine that supports breathing. The bacteria and viruses that most commonly cause pneumonia in the community are different from those in healthcare settings.
That was amazingly clear for something from the CDC, so I assume Todd the Intern was on vacation and his boss had to do some work for a change. They certainly didn’t get this long of an intelligible statement out of Nate.
The important bits here are:
There are different pathogens found in community-acquired pneumonia vs. hospital-acquired
There are enough cases of hospital-acquired and ventilator-associated pneumonia that these are their own categories.
Let’s talk about CAP
Community-acquired pneumonia (CAP) is not as well understood as we might like.
Diagnosis and Treatment of Adults with Community-acquired Pneumonia(Metlay et al 201912):
CAP is an extraordinarily heterogeneous illness, both in the range of responsible pathogens and the host response.
This reference is a detailed (23 pages and 216 references) guide on how to determine what type of pathogen is involved, and how to treat it. At the end, the authors emphasize how many unknowns still remain:
It remains disappointing how few key clinical questions have been studied adequately enough to allow for strong recommendations regarding the standard of care.
How about hospital-acquired pneumonia?
I didn’t even know this was a thing until Nate had too many vodka tonics one night and spilled the beans.
The epidemiology of nonventilator hospital-acquired pneumonia in the United States (Giuliano, Baker, and Quinn 201713)
Hospital-acquired pneumonia, both with and without a ventilator, accounts for a lot of health care-acquired infections.
Hospital-acquired pneumonia (HAP) is a common health care-acquired infection (HAI) worldwide, occurring at a rate of up to 21 cases per 1,000 hospital admissions. HAP includes 2 distinct sub-groups: nonventilator HAP (NV-HAP) and ventilator-associated pneumonia (VAP). Results from a multistate point-prevalence survey using the National Healthcare Safety Network criteria for HAIs suggest that NV-HAP and VAP combined accounted for 21.8% (95% confidence interval, 18.4-25.6) of all HAIs in the United States during 2011.
So in the survey it was about one fifth of the health care-acquired infections. And these infections had a high mortality rate:
Our mortality rate of 13.1% is consistent with the NV-HAP mortality ranges of 13.9%-30% reported by other researchers. Although the odds of death for patients with NV-HAP were significantly lower than patients with VAP, the absolute number of patient deaths from NV-HAP in our sample was 15,593 compared with 631 patients with VAP. Thus, the overall mortality influence associated with NV-HAP was much greater than VAP, a finding consistent with previous research.
Ventilators seem kind of dangerous, if used improperly. That’s probably why the hospital won’t let me play with them.
Like all good tools, ventilators are useful but can also be dangerous - when using a ventilator the benefits must be balanced against the risks.
Ventilator-associated pneumonia in adults: a narrative review (Papazian et al. 202014)
Ventilator-associated pneumonia (VAP) is defined by infection of the pulmonary parenchyma in patients exposed to invasive mechanical ventilation for at least 48 h and is part of ICU-acquired pneumonia. VAP
remains one of the most common infections in patients requiring invasive mechanical ventilation.
So a lot of people who are put on ventilators for an extended period of time get pneumonia. How common is this?
VAP is reported to affect 5–40% of patients receiving invasive mechanical ventilation for more than 2 days, with large variations depending upon the country, ICU type, and criteria used to identify VAP.
Choose your hospital wisely, I guess. How dangerous is VAP?
Based on aggregate data from 58 randomized studies on VAP prevention, the estimated attributable mortality rate of VAP was 9%. A similar approach using individual patient data for meta-analysis, including 6284 patients from 24 VAP prevention trials, estimated an attributable mortality of 13%…
The authors also tell us what things reduced VAP the most.
The prevention practices that have most consistently been associated with improving objective outcomes for ventilated patients have been those focused on avoiding intubation and minimizing exposure to invasive ventilation by using high flow oxygen or noninvasive ventilation as alternatives to intubation, lightening sedation, using spontaneous breathing trials to prompt early extubation, and early mobilization.
So try to avoid sticking tubes down people’s throats, ease up on the drugs, give them oxygen, do breathing exercises, and try and get them moving. This is eerily similar to the instructions I have to give Nate before he goes to those wild parties that wind up with someone sleeping on the front lawn.
Okay so neither me nor Nate should mess with ventilators. Anything else we should know?
Sometimes a suspected case of VAP turns out to be something called Aspergillosis instead (which is classified separately in the ICD codes, so not included in the CDC table at the top of this post). It’s caused by a common but often missed pathogen, Aspergillus fumigatus.
Pulmonary Aspergillosis in Patients with Suspected Ventilator-associated Pneumonia in UK ICUs (Laughlin et al. 202015)
Of 194 patients evaluated, 24 met the definition of probable Aspergillus infection, giving an estimated prevalence of 12.4%.
The authors point out that 12.4% is higher than expected based on other data but that Aspergillus infections might be missed frequently.
Aspergillosis is consistently found to be among commonly missed diagnoses in critically ill patients, demonstrated by the results of multiple autopsy studies.
For agents casting Aspergillosis public service announcements, Nate refers his friend Irene the Invasive Pulmonary Aspergillosis Aardvark. Her name is a bit of a mouthful but Irene IPA just sounds like a brand of beer.
So where the heck am I going with all this?
COVID-19 is currently classified as a type of pneumonia. A lot of cases of pneumonia involve secondary infections that occur after a viral infection and these secondary infections are often the actual cause of death.
Some pneumonia involves multiple pathogens (viral, bacterial or fungal) and treating one or more of those pathogens may lead to improved outcomes.
Putting patients on ventilators may be necessary in some cases, but it may also cause a secondary infection and these are often fatal as well.
And given what we now know about pneumonia and ICD codes, the CDC’s presentation of the data creates more questions than it answers. For example (and this is only a partial list):
For how many deaths “involving” COVID-19 was it the primary cause?
For how many of those was the COVID-19 confirmed vs. presumed?
Does it include people with COVID-19 and something like Aspergillosis, that’s not included under pneumonia?
How many cases of pneumonia of unknown cause have been categorized as COVID-19, but could have been something else?
In the deaths involving COVID-19 and pneumonia, what was the actual cause of death?
Do some of these have multiple causes of death listed?
Since, more often than not, we don’t know the pathogen responsible for pneumonia deaths, how do we really know how many of deaths are due to COVID-19? What if many of them are due to secondary infections, that if treated, would not have resulted in death?
Is this why some doctors have been trying things like broad spectrum antibiotics, antivirals, and drugs like Ivermectin? For example, some doctors have been prescribing doxycycline, which is often given to patients with community-acquired bacterial pneumonia.
After almost two years of frantic government responses, we deserve better data and better answers.
And, quite frankly, a sober spokes-gnome.
It’s been a few days since my last post, mostly because pneumonia really is a very difficult topic. And a little bit because of an alcoholic gnome.
We’re getting into more difficult topics and it’s important to be as accurate and useful as possible, otherwise what’s the point of doing this at all? The internet is 99.999999999% useless garbage and I prefer not to add another digit to that.
https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
Wang Y, Wang Y, Chen Y, Qin Q. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J Med Virol. 2020;92(6):568-576. doi:10.1002/jmv.25748
https://pubmed.ncbi.nlm.nih.gov/32134116/
A zip file containing the code tables can be found at this link:https://www.cms.gov/medicare/icd-10/2022-icd-10-cm
Kaysin A, Viera AJ. Community-Acquired Pneumonia in Adults: Diagnosis and Management. Am Fam Physician. 2016 Nov 1;94(9):698-706. Erratum in: Am Fam Physician. 2017 Apr 1;95(7):414. PMID: 27929242.
https://pubmed.ncbi.nlm.nih.gov/27929242/
https://www.aafp.org/afp/2016/1101/p698.html
Musher DM, Abers MS, Bartlett JG. Evolving Understanding of the Causes of Pneumonia in Adults, With Special Attention to the Role of Pneumococcus. Clin Infect Dis. 2017 Oct 30;65(10):1736-1744. doi: 10.1093/cid/cix549. PMID: 29028977; PMCID: PMC7108120.
https://pubmed.ncbi.nlm.nih.gov/29028977/
Mandell LA. Community-acquired pneumonia: An overview. Postgrad Med. 2015 Aug;127(6):607-15. doi: 10.1080/00325481.2015.1074030. PMID: 26224210; PMCID: PMC7103686.
https://pubmed.ncbi.nlm.nih.gov/26224210/
NIH page about pneumonia:
https://www.nhlbi.nih.gov/health/pneumonia
Archived copy:
https://web.archive.org/web/20211202212635/https://www.nhlbi.nih.gov/health/pneumonia
Reynolds JH, McDonald G, Alton H, Gordon SB. Pneumonia in the immunocompetent patient. Br J Radiol. 2010 Dec;83(996):998-1009. doi: 10.1259/bjr/31200593. PMID: 21088086; PMCID: PMC3473604.
https://pubmed.ncbi.nlm.nih.gov/21088086/
Medical dictionary definition of parenchyma:
https://medical-dictionary.thefreedictionary.com/parenchyma+of+lung
Archived copy:
https://web.archive.org/web/20211204053427/https://medical-dictionary.thefreedictionary.com/parenchyma+of+lung
Mackenzie G. The definition and classification of pneumonia. Pneumonia (Nathan). 2016;8:14. Published 2016 Aug 22. doi:10.1186/s41479-016-0012-z
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5471962/
CDC page on pneumonia:
https://www.cdc.gov/pneumonia/causes.html
Archived copy:
https://web.archive.org/web/20211204055439/https://www.cdc.gov/pneumonia/causes.html
Metlay JP, Waterer GW, Long AC, Anzueto A, Brozek J, Crothers K, Cooley LA, Dean NC, Fine MJ, Flanders SA, Griffin MR, Metersky ML, Musher DM, Restrepo MI, Whitney CG. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019 Oct 1;200(7):e45-e67. doi: 10.1164/rccm.201908-1581ST. PMID: 31573350; PMCID: PMC6812437.
https://pubmed.ncbi.nlm.nih.gov/31573350/
Giuliano KK, Baker D, Quinn B. The epidemiology of nonventilator hospital-acquired pneumonia in the United States. Am J Infect Control. 2018 Mar;46(3):322-327. doi: 10.1016/j.ajic.2017.09.005. Epub 2017 Oct 16. PMID: 29050905.
https://pubmed.ncbi.nlm.nih.gov/29050905/
Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: a narrative review. Intensive Care Med. 2020 May;46(5):888-906. doi: 10.1007/s00134-020-05980-0. Epub 2020 Mar 10. PMID: 32157357; PMCID: PMC7095206.
https://pubmed.ncbi.nlm.nih.gov/32157357/
Loughlin L, Hellyer TP, White PL, McAuley DF, Conway Morris A, Posso RB, Richardson MD, Denning DW, Simpson AJ, McMullan R. Pulmonary Aspergillosis in Patients with Suspected Ventilator-associated Pneumonia in UK ICUs. Am J Respir Crit Care Med. 2020 Oct 15;202(8):1125-1132. doi: 10.1164/rccm.202002-0355OC. PMID: 32609533; PMCID: PMC7560800.
https://pubmed.ncbi.nlm.nih.gov/32609533/