

A Theory on Regulatory Oversight
A Theory on Regulatory Oversight
Does anyone seriously think this is a coincidence?

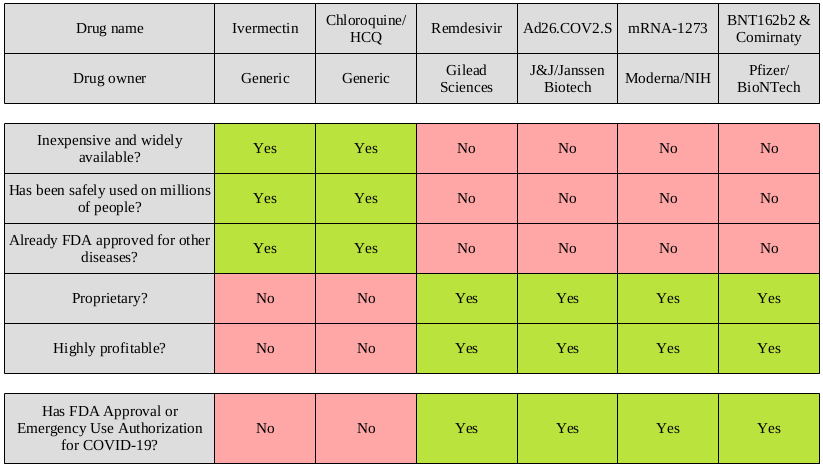
I made a fun little chart. It lists six different suggested treatments for COVID-19, and there might be a pattern. It’s really subtle so I can understand how journalists have missed it up till now.
And maybe, just maybe, I have a way to explain this pattern. I call it the Hookers and Blow Theory of Pharmaceutical Regulation.
Ivermectin
As discussed in a previous post about Ivermectin, it was originally developed to treat parasitic diseases and was approved for human use in 1987. Close to 4 billion doses have been administered, to millions of people, with few if any adverse events. But nobody makes money on it because only poor people get parasitic diseases.
Although not currently approved as an antiviral, multiple teams of researchers have conducted lab tests that demonstrated antiviral properties on viruses like dengue and yellow fever.
Sounds like a great candidate for Emergency Use Authorization - except the patents expired and the drug will never generate enough money to hire one, let alone multiple, hookers. And absolutely no blow.
No one is applying for an EUA, and on their own the FDA regulators are basically useless. No authorization for Ivermectin.
Chloroquine/Hydroxychloroquine
Chloroquine has been used to treat malaria since the 1940s, when cocaine parties were still a novelty. Researchers have lab tested it (Chloroquine, not cocaine) on SARS-CoV-2 with promising results. Hydroxychloroquine is similar but a little less toxic, although both are much safer than coke when taken in the correct dosage.
But neither drug will ever generate “hookers and blow” money so the FDA will continue to ignore both of them.
Remdesivir
Remdesivir, a new broad spectrum antiviral drug, was originally tested on Hepatitis C and RSV (Respiratory Syncytial Virus) but it failed to demonstrate efficacy against those viruses. It was then repurposed for treatment of Ebola but hasn’t been approved to treat it. That’s okay though, it’s proprietary so we’ll keep re-purposing until we find a purpose.
Just like Ivermectin and Chloroquine, lab testing has shown potential for the treatment of COVID-19. Unlike the other two drugs, the FDA somehow found it in their hearts to grant Emergency Use Authorization to this little money maker.
This is clearly because of the incredible therapeutic potential of Remdesivir and not because it could potentially generate enough cash to drown the inventors in a mountain of coke.
J&J/Janssen Biotech Ad26.COV2.S
Ad26.COV2.S is an adenovirus-based vaccine. Adenovirus has been used as a vector for gene therapy, and has been studied as a vaccine vector. An adenovirus-based vaccine was recently approved in the European Union for the treatment of Ebola, and vaccines for influenza and HIV-1 are being studied.
This is exciting technology, although not exactly with a long track record of widely used vaccines. But when the FDA held their big meeting and the monkey threw the dart, it landed on Ad26.COV2.S.
The fact that the vaccine is proprietary and profitable is simply coincidental.
Moderna/NIH mRNA-1273
Messenger RNA! It’s new, it’s exciting, and Moderna can afford a clinical trial with 30,000 subjects! Moderna did have help from the NIH to develop the vaccine, so you would think it was at least partially public property, but you would be wrong.
The FDA decided to grant EUA because of the vast potential of this technology, a decision not at all influenced by the potential money and/or limos full of hookers.
Pfizer/BioNTech BNT162b2 and Comirnaty
This one is also mRNA and Pfizer has even more cash than Moderna - their clinical trial had 44,000 subjects. Their original version (BNT162b2) was given EUA, but Pfizer went the extra mile and when they call it Comirnaty it has actual FDA approval rather than just emergency authorization.
Good luck getting some of the Comirnaty though, because they don’t have immunity from liability for that version. But they get the public relations bump from having something with the words “approved” associated with their product.
[The fact that everyone keeps confusing BNT162b2 with Comirnaty has absolutely nothing to do with Pfizer advertising money paying the salaries of journalists reporting about it.]
Emergency Use Authorization and Biologics License Application Approval - once again the nod goes to the product with the big jackpot. We all yearn to be loved as much as the FDA loves Pfizer.
Your FDA: somehow even worse than useless
It kinda sorta seems like maybe the FDA doesn’t care about a treatment unless it’s capable of generating private jet and airstrip money.
Keep in mind this is just a theory, and there could be other reasons. For example, if we allowed Emergency Use Authorization for really cheap, readily available drugs, then doctors might try those options. Clearly this is morally wrong.
It’s also unfortunate that we don’t have any kind of publicly funded health agency that could conduct studies, like randomized controlled trials, on the cheap drugs right from the beginning.
But all we have are groups like the FDA, the CDC, and the NIH - tiny little agencies with billion dollar budgets but apparently no expertise in medical studies.
Maybe someone will figure out how to re-patent something like Ivermectin so it becomes really expensive, prompting the FDA to grant it Emergency Use Authorization too. In the meantime we’ll need to make do with the unfortunately expensive treatments instead.
The boring academic part
What’s occurring here is an example of something called regulatory capture. Check out my article On regulatory capture for an explanation, and a brief discussion of a published paper on this subject.
(Note: The subject is academic. My explanation is, well, a typical example of how I explain things.)
Beautiful! Thank you for this most accurate assessment. And I love the little chart. It really lays out the issue with great clarity.
This is a very nice article. Thank you!
There is a recent adversarial result on Ivermectin (ACTIV-6 study) showing some benefit. Alexandros Marinos wrote excellent pieces:
https://doyourownresearch.substack.com/p/activ-6-trial-ivermectin-scientists
https://doyourownresearch.substack.com/p/activ-6-dosing-and-timing-a-fox-in
I also added my two cents: https://norstadt.substack.com/p/ivermectin-seems-to-have-benefits